- Visibility 187 Views
- Downloads 40 Downloads
- Permissions
- DOI 10.18231/j.jdpo.2024.039
-
CrossMark

Angiolipoleiomyoma of uterus, a rare subtype of leiomyoma - A case report
- Author Details:
-
 Jayalakshmy P S *
Jayalakshmy P S *
-
Ayisha shaheeda Cherukattil
-
Muhsina Mohamed Rasif
Abstract
Angiolipoleiomyoma is a rare benign mesenchymal tumour. It can occur in various organs like skin, soft tissue kidney and genital tract. Here, we are reporting a case of Angiolipoleiomyoma of uterus in a 54-year-old patient.
Introduction
Angiolipoleiomyoma (ALLM), a rare benign mesenchymal tumour is considered as a subtype of uterine leiomyoma (LM). This may be mistaken for angiomyolipoma (AML), a tumour belonging to the perivascular epithelioid cell family of tumours (PEComa). The latter is most often associated with Tuberous sclerosis whereas ALLM has no such association. Hence, awareness of the existence of this morphological subtype of LM is essential for the pathologists in order to avoid misdiagnosis of the lesion.
Case presentation
A 54-year-old female patient, G5P5L5, presented with right sided lower abdominal pain and intermittent bleeding per vagina since last 5 months. No comorbidities detected. Magnetic resonance imaging (MRI) showed a solid lesion with tiny cystic spaces measuring 3.5x3cm in the right cornual region of the fundus of uterus. One submucosal and one intramural fibroid were also noted. Total abdominal hysterectomy with bilateral salpingo-oopherectomy was done with a clinical diagnosis of parametrial / ovarian lesion. The postoperative period was uneventful.
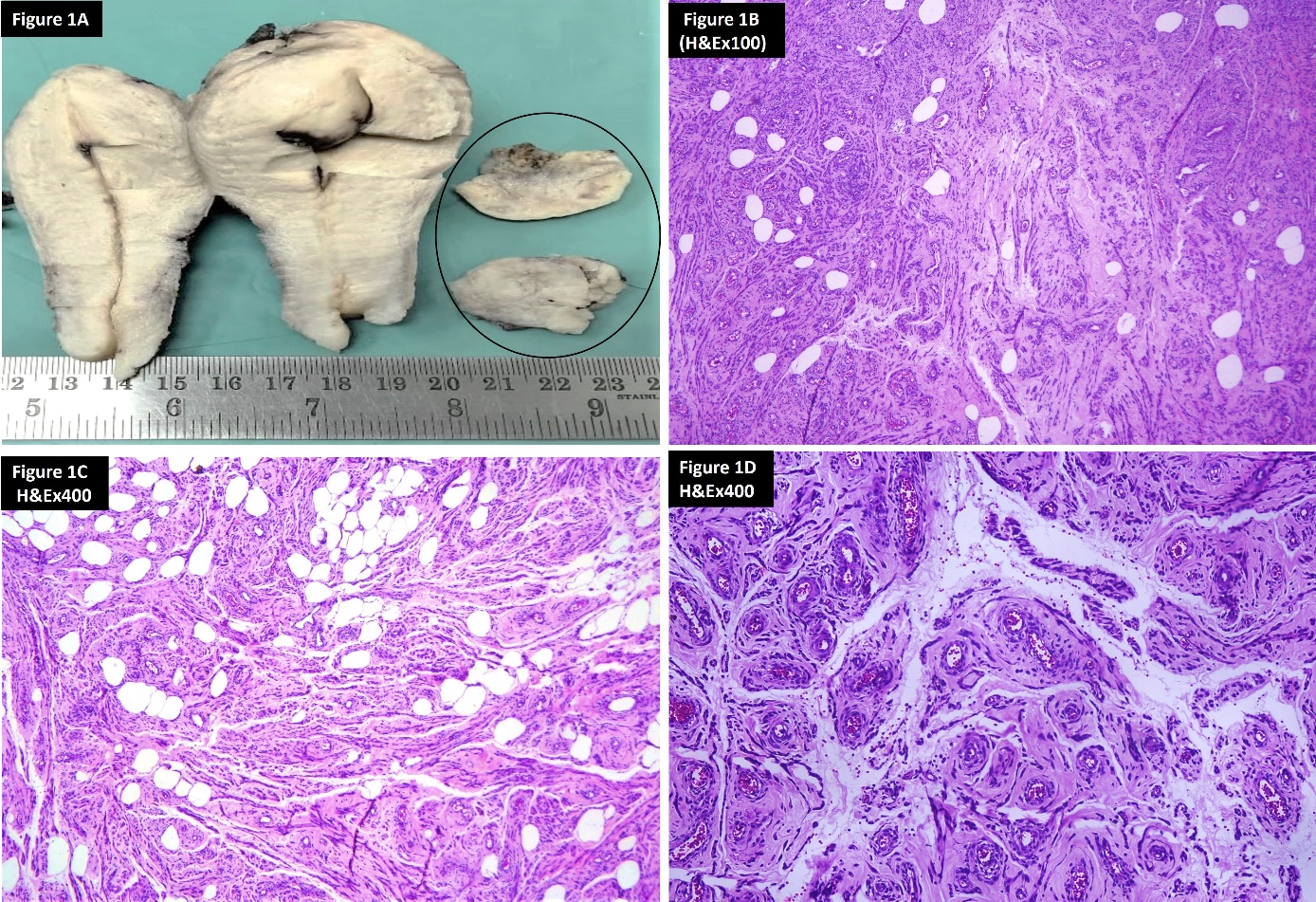
Specimen of total hysterectomy with bilateral salpingo-oophectomy and the right cornual lesion as separate nodular mass was received in our pathology department. The cornual mass measured 2.5x2.5x1.7cms. Outer surface of this mass was pale brown, irregular. Consistency was soft to firm. On cutting, the mass was pale brown to yellow with microcystic spaces some containing dark coloured fluid inside. There was no significant whorled appearance of a usual leiomyoma. Uterus was globular and showed a defect in the fundus near right cornu. On sectioning, showed a submucosal fibroid measuring 2.5x2x2cms and an intramural fibroid measuring 3x2.5x1cms, both of which showed the typical whitish whorled appearance of leiomyoma. Both ovaries and fallopian tubes were of unremarkable gross appearance.([Figure 1]A)
On histological examination, the mass showed a circumscribed neoplasm with three components, smooth muscle fibres admixed with numerous thick-walled vessels of varying sizes and mature adipocytes. No nuclear atypia, mitosis or necrosis noted within any of the three components of the tumour. ([Figure 1]B-D) Masson trichrome stain highlighted the smooth muscle fibres (red) interspersed with abundant collagen (green). ([Figure 2]D) Hence, a diagnosis of angiolipoleiomyoma was considered morphologically. Uterus had also one submucosal and one intramural leiomyomas. Both ovaries and fallopian tubes histologically were normal.
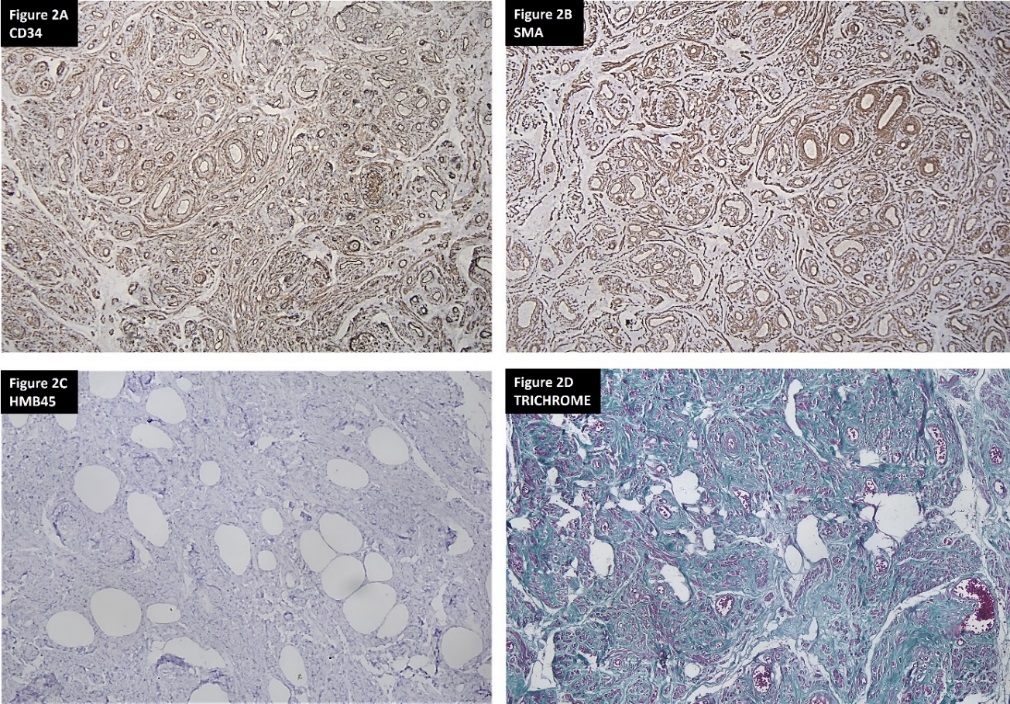
For confirmation of the morphological diagnosis and to rule out the possibility of AML, a tumour of PEComa family which is a close morphological mimicker, immunohistochemistry (IHC) was done with anti HMB45, anti SMA and anti CD34. HMB45 was negative in the tumour ruling out the possibility of angiomyolipoma. SMA was positive in the smooth muscle component, CD 34 highlighted the vessels, thus confirming the diagnosis of ALLM.([Figure 2]A-C)
Discussion
ALLM, a rare mesenchymal tumour is considered to be a subtype of leiomyoma. Only around 21 cases have been reported in the English literature. [1] This tumour has been reported in skin, kidney, soft tissue and several other organs. In the uterus, this tumour is usually seen in the body of the uterus but, may be seen in the cervix or lower uterine segment. It can be intra mural or subserosal as in the case of classic leiomyoma. The size may vary from small to very large replacing the uterine myometrium. The tumour size ranged from 2 to 16 cm with a median of 8.4 cm in one study. [2] It can be encapsulated with a pseudocapsule or may be infiltrative. The nomenclature of this tumour is controversial. Some authors think that this is a hamartomatous lesion. [3] Cases of AML have been reported in uterus.[4] Hence some authors opine that ALLM is an extra renal AML.
Histologically ALLM shows three tissue components- smooth muscle, blood vessels and mature adipose tissue in varying proportion as in AML, the PEComa tumour. Current concept is that this tumour is a subtype of classic leiomyoma. Many subtypes of uterine LM have been described in WHO blue book and other standard surgical and gynaecological pathology books like angioleiomyoma, lipoleiomyoma, mitotically active LM, Symplasmic LM etc. Angio LM & lipo LM has only one component apart from the smooth muscle cells. But in ALLM, these three tissue components are intimately intermixed. Some times ALLM can show degenerative nuclear atypia just like symplasmic leiomyoma as was seen in the case described by Ren RL et al. [2]
Both ALLM and AML histologically shows a mixture of smooth muscle cells, adipocytes and blood vessels. Regarding immunoprofile, both ALLM and AML can be positive for smooth muscle and vascular markers, but, ALLM is almost always negative for HMB 45 which is the immunomarker for the AML and other PEComa group of tumours. Moreover, in various reports, none of these cases were associated with tuberous sclerosis, the association being common in cases of AML.
Camille verocq et al. has reported a case of ALLM with KRAS and KIT mutation. [5] Whether this is a recurrent mutation specific for this tumour or not is not established. Reporting of more cases and molecular study of these cases are needed to determine this. ALLM has been recently reported in association with a dermoid cyst in the ovary by Gupta et al.[6] This was a large lobulated mass measuring 23 cm in greatest diameter almost replacing the uterus with a simultaneous dermoid cyst in the right ovary. Handler et al. reported a case of consumptive coagulopathy secondary to a large degenerated ALLM. [7]
Several studies have proposed that this tumour has to be categorized as a benign leiomyoma subtype and included in the World Health Organization classification of tumours of the female genital tract.[8], [9] The authors are also of the same opinion that this tumour is a benign subtype of leiomyoma since it shows morphological and immunophenotype of smooth muscle; with admixture of the angiomatous and lipomatous component. Whether these components are metaplastic or a clonal proliferation, as part of the tumour has to be ascertained with large scale study of this type of tumour. As of now it is not possible since only a few cases have been reported till date. We have to wait till enough cases are reported for a large-scale research and establishing the exact nature of this lesion.
Conclusion
A case of angiolipoleiomyoma is reported in the uterus of a 54 year old female. This is to be considered as a benign subtype of leiomyoma since it shows the features of leiomyoma morphologically and in the immunoprofile. The authors think that reporting of rare cases is necessary to add up the number of cases in the literature so that more studies can be done in such poorly understood entities. If more cases are reported from various part of the world, after adequate study, this may be added to the WHO classification of tumours in the next edition and the entity will find its place in other standard and specialised text books.
Consent for Publication
Consent has been obtained from the patient.
Conflict of Interest
None.
Source of Funding
None.
References
- Sulkar S, Swami S. Angiolipoleiomyoma [ALLM] of uterus: A rare case report. Int J Clin DiagnPathol. 2022;5(1):32-4. [Google Scholar]
- Ren R, Wu H. Pathologic quiz case: A 40-year-old woman with an unusual uterine tumour. Arch Pathol Lab Med. 2004;128(2):31-2. [Google Scholar]
- Mckeithen S, Shinner J, Michelsen J. Hamartoma of the uterus, report of a case. Obstet Gynec. 1964;24:231-4. [Google Scholar]
- Wang J, Yang Q, Zhang N, Wang D. Uterine angiomyolipoma: a clinical analysis of 8 cases and literature review. Arch Gynecol Obstet. 2021;304(1):171-7. [Google Scholar]
- Verocq C, Noël J, Ouertani S, D'Haene N, Catteau X. First Case Report of a Uterine Angiolipoleiomyoma With KRAS and KIT Mutations. Int J Gynecol Pathol. 2022;41(6):578-82. [Google Scholar]
- DG, Malhotra P, Rahar S, Ahuja A. Angiolipoleiomyoma of the Uterus with a Dermoid Cyst in the Right Ovary: An Unusual Association. J Midlife Health. 2024;15(2):104-6. [Google Scholar]
- Handler M, Rezai F, Fless KG, Litinski M, Yodice P. Uterine angioleiomyoma complicated by consumptive coagulopathy. Gynecol Oncol Case Rep. 2012;142(4). [Google Scholar]
- Garg G, Mohanty S. Uterine angioleiomyoma: a rare variant of uterine leiomyoma. Arch Pathol Lab Med. 2014;138(8):1115-8. [Google Scholar]
- Zizi-Sermpetzoglou A, Myoteri D, Arkoumani E, Koulia K, Tsavari A, Alamanou E. Angioleiomyoma of the uterus: report of a distinctive benign leiomyoma variant. Eur J Gynaecol Oncol. 2015;36(2):210-2. [Google Scholar]